

")
")

Ambulatory operations
The advantages of ambulatory operationsHospitalisation is no longer necessary for a number of operations. The main advantage of ambulatory operations is the level of trust in your doctor, your surgeon of choice, who is familiar with your condition and will also be responsible for post-operative treatment. Treatment is more individually suited to the patient and everything is in one hand. In the ambulatory process you know the experienced specialist consultant who is carrying out the operation. Modern anaesthetics mean that there is principally no age limit. Patients undergoing an ambulatory anaesthetic or narcosis are selected by the anaesthetist in accordance with strict regulations. Modern clinical standards are also ensured for all aspects of ambulatory operations. Following an operation, patients are generally far more mobile than is assumed by those have never undergone surgery. Recovery in the home environment is quick and without complications, indeed, often better than in hospital. There is decidedly less emotional stress involved, particularly for children and older people. They are spared the stay in unfamiliar surroundings. In the USA and England more than half of all operations are ambulatory. In view of the increasing cost of health care, the call for “as much outpatient care as possible” is the motto of all cost-conscious health care politicians. Ambulatory operations are definitely cheaper and better for the tight budget of the health service. |
Ambulante Operationen finden unter strengen Sicherheitsbedingungen statt. Dafür sorgen neben gesetzlichen Vorschriften vor allem Qualitätsrichtlinien der Ärztlichen Zentralstelle Qualitätssicherung (ÄZQ) und des Bundesverbandes für Ambulantes Operieren (BAO). Ambulatory operations we carry out in the surgical OP-Zentrum Berlin Reinickendorf. |



Ambulatory operations
The handA further focus of ambulatory operations is hand surgery. All hand surgery is ambulatory and a local or regional anaesthesia is given whenever possible. Below are some frequent hand disorders that may require surgery due to their duration and the failure of orthodox treatment. Patients with a carpal tunnel syndrome have no feeling in the fingers, usually during the night. Over time, fine motoric disturbances arise and there may be loss of strength. This is caused by restriction of the median nerve in the area of the carpal bones. The overlying ligament is split in an operation, allowing the nerve more space. The symptoms should already have disappeared by the first night after the operation. Trigger finger syndrome: whereby one finger cannot be extended again after bending. The tendon becomes trapped in the tendon sheath at the base of the finger, causing pain and inhibiting movement. The condition ceases when the tendon sheath is surgically split. Dupuytren´s contracture: the subcutaneous layer of tissue (fascia) in the hand becomes hardened or shrinks and progressively pulls the fingers into the palm of the hand. This usually affects the ring and small finger. Although this disease should not be operated on in the early stage (formation of small lumps in the palm) |
surgical treatment should not be put off too long as otherwise serious limitations to movement will occur. Bible bump or ganglion cyst: this is a swelling that can develop on the back on the hand, the wrist or the tendon sheath of flexor muscles. It is usually caused by a relative weakness of the joint capsule, which fills with synovial fluid that then thickens in the ganglion putting pressure on the surrounding tissue. Tears to tendons of the hand and fingers usually have to be surgically treated in order to maintain the functions of the hand. |

Ambulatory operations
Arthroscopic meniscus operationsA meniscus tear has been diagnosed on the basis of your description of your knee problems and clinical examinations i.e. performing certain provocative manual tests. The medial and lateral menisci are sickle-shaped discs of cartilage between the thigh and shin bones, which serve to absorb shock and stabilise the knee joint. In the case of injury, such as rotation during sport or due to joint degeneration in advanced age, a meniscus may tear and parts of it become deposited in the joint-space. The results is pain on moving and when putting weight on the knee, as well as mechanical damage to the joint cartilage. The aim of the arthroscopic meniscus operation is to remove all torn particles while preserving undamaged meniscus tissue. Only those parts are removed that inhibit the joint function, damage the joint surfaces or cause pain and inflammation. This is done using miniature instruments that have been especially developed for arthroscopic orthopaedics and surgical cutting instruments with a vacuum feature. In some cases it is possible to arthroscopically suture the meniscus, for example when the tear is very close to the capsule. Removal of the meniscus is then no longer necessary. Welcome side-effects of arthroscopic orthopaedics are the almost complete absence of pain following the operation, the lack of large scars and the possibility of carrying out ambulatory operations. As mentioned above, the main advantage of the arthroscopic technique over ‘cutting operations’ is that all intact parts of the meniscus can be left untouched. |
Arthroscopic resection of the meniscus therefore considerably reduces the risk of the occurrence of postoperative arthritis. The operation requires an incision no longer than 0.2 of an inch through which a camera, and any equipment that may be needed, is inserted into the joint. Irrigation fluid is pumped into the joint to distend the space between its surfaces and ensure a good view. Meniscus tears, for example, are sutured if possible and medically sensible, otherwise partially or entirely removed. |

Ambulatory operations
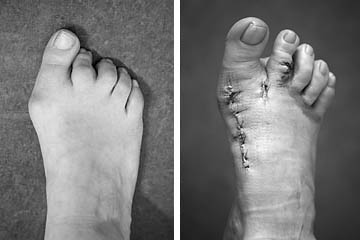
The footAccording to statistics, about 50% of the adult population of Central Europe have painful or deformed feet or toes. |
|
Ambulatory operations
Arthroscopic operations for arthrosis and damaged cartilageCartilage damage can occur in the knee as a result of injury, overexertion or due to mechanical functions. Four stages can be differentiated:
Cartilage damage can occur on the cartilaginous joint surfaces of the thigh and shines through mechanical disturbance caused by an old meniscus tear. Minimal incarcerations of meniscus particles between the joint surfaces cause fraying, which can progress to complete abrasion of the cartilaginous surface. The prognosis, with regard to load-bearing capacity and freedom from symptoms following arthroscopic operation of a meniscus, depends on the damage caused to the cartilage by the injury. Frayed and shredded cartilage is smoothed using special arthroscopic cutting instruments with a vacuum function. All loose particles are sucked out of the joint. Depending on the extent of the findings, the patient needs elbow crutches to keep the weight off the leg for 1 – 4 weeks following the arthroscopic operation. If there is already complete abrasion of the joint cartilage, treatment involves freeing the bone from dead superficial tissue in order to trigger cartilage production. Using a surgical shaving instrument the bone is superficially shaved until the blood supply to the bone is visible. This is the only method that facilitates the development of new cartilage-like tissue from within the depth of the shaved bone in 3-6 months, and which is capable of taking over much of the function of the lost joint cartilage. In order to allow the covering layer to become as thick and durable as possible the patient has to use elbow crutches for approx. 6 weeks following the arthroscopic operation. This means that the operated knee only carries out walking movements without taking any weight. We will teach you how to walk using crutches and are sure that you will find it simple to learn. |
Production of replacement fibrocartilage (microfracture according to Steadman, subchondral abrasion, Pridie drilling):In the case of complete cartilage lesion of the subchondral bone the aim of the repair process is to provide fibrocartilage cover for the damaged chondral surface. Perforation of the hard bone layer causes blood and bone marrow cells to flow into the damaged cartilage. Some of the released cells are pluripotent i.e. undefined, and still able develop into specialist cells. The direction of their development is determined by the nature of the surrounding area. This means that in an area of damaged cartilage the cells receive information to become cartilage cells and then produce new, replacement fibrocartilage. The type of cartilage damage determines which process is applied.
|

